

Abstract
Introduction: JAK2V617F mutation is one of the major criteria in the diagnosis of myeloproliferative neoplasms (MPN). The disease phenotype and outcomes are dependent on variant allele fraction (VAF) of JAK2V617F. Recently, a new entity termed clonal hematopoiesis of indeterminate potential (CHIP) defines patients with normal cell counts and VAF of at least 2%. Outcomes of patients with <2% VAF are scarce and we aimed to retrospectively study characteristics and outcomes of patients with JAK2V617F VAF < 2% compared to patients with VAF 2-10%.
Methods: The study population included all patients in the province of British Columbia with JAK2V617F testing performed during 2010-2015. We compared the patient characteristics, disease phenotypes, overall survival (OS), thrombosis-free survival (TFS) and cumulative incidence of thrombotic events between patients with VAF <2% and 2-10%. Parallel real-time quantitative polymerase chain reaction (RQ-PCR) for wild type JAK2 and JAK2V617F was used as detection method. MPN diagnoses were based on the treating physicians' assessment.
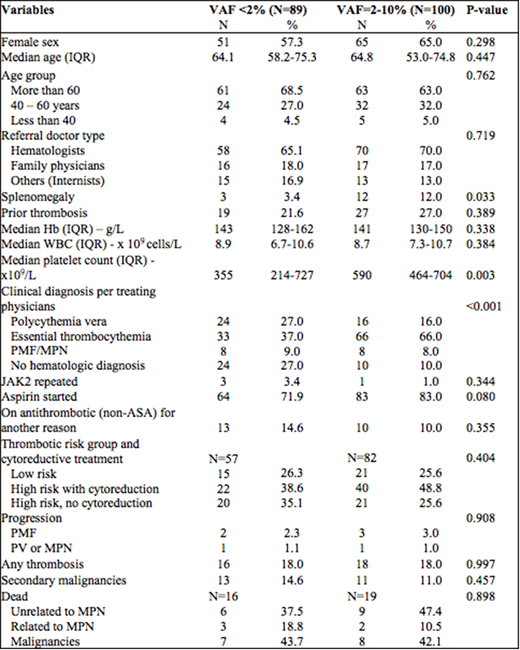
Results: We identified 216 patients with JAK2V617F VAF < 10%. Twenty-seven patients were excluded due to missing follow-up data. A total of 189 patients were included for final analysis (89 patients with VAF <2% and 100 patients with VAF 2-10%). Patient characteristics, diagnoses and outcomes are shown in the Table. Patients with JAK2V617F >2% have significantly higher rate of splenomegaly, higher platelet counts and higher MPN diagnoses. Ten patients (10.0%) with VAF 2-10% had no hematologic diagnoses, consistent with CHIP, while 24 patients (27.0%) with VAF <2% had no hematologic diagnoses. There were no differences in all outcomes measured including thrombotic complications, progression to hematologic or solid cancers and death. The median follow-up time for the whole cohort was 5.2 years with interquartile range (IQR) 3.5-6.6 years. The 5-year OS were 81.0% for VAF < 2% and 81.7% for VAF 2-10%, log-rank P = 0.922. TFS at 5 years were 71.2% and 69.5%, respectively (P = 0.982). The 5-year cumulative incidences of thrombotic complications (considering death as a competing event) were 8.8% and 11.3%, respectively (Pepe-Mori P = 0.574).
Further analysis by clinical diagnoses classified patients into polycythemia vera (PV) 40 (21.2%), essential thrombocythemia (ET) 99 (52.3%), primary myelofibrosis or MPN, NOS (PMF/MPN) 16 (8.5%) and clonal hematopoiesis of indeterminate potential (CHIP) or no hematologic diagnosis 34 (18.0%). Patients with PMF/MPN were significantly older than patients with other diagnoses (median age PV 64.2, ET 64.3, PMF/MPN 80.7 and CHIP 54.1 years, P=0.019). The 5-year OS were: PV 91.4%, ET 90.0%, PMF/MPN 31.3% and CHIP/no hematologic diagnoses 58.7%, P<0.001. TFS at 5 years were 83.1%, 74.7%, 25.0%and 57.4%, respectively, P<0.001.
Conclusion: Patients with JAK2V617F VAF < 2% have less splenomegaly and are less likely to have a diagnosis of MPN compared to patients with VAF 2-10%. However, the incidence of thrombotic events was similar between patients with VAF < 2% and 2-10%. In the combined VAF < 10% cohort, PMF/MPN patients were older and had the worst survival outcomes. The mortality in this PMF/MPN group was mostly unrelated to MPN diagnoses. Interestingly, patients with CHIP/no hematologic diagnoses in this study have the next worse OS and TFS. This could be explained by selection bias for performing JAK2 testing in acute or chronically ill patients with reactive changes in the peripheral blood.
Foltz:Gilead: Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Promedior: Research Funding; Incyte: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal